
A woman standing with fruit baskets ready for sale in Hanoi, Vietnam from unsplash
When the City Shapes the Mind: Understanding NCDs Through Urban Stress
In cities where stress is constant, the mind adapts and those adaptations shape how people eat, cope, and stay healthy
PUBLIC HEALTH
by Alexandra Dowding
24th May 2026N
on‑communicable diseases (NCDs) such as diabetes, cardiovascular disease, and hypertension, now account for around 80% of global deaths, with around 73% occurring in low‑ and middle‑income countries (LMICs). As urbanisation accelerates across South Asia, Southeast Asia, Latin America, the Middle East,
and Africa, daily life in LMIC cities is increasingly shaped by structural pressures: insecure housing, long commutes, food insecurity, income volatility, and exposure to violence.
These stressors are not simply social conditions; they are physiological exposures that shape cognitive bandwidth, planning capacity, and the coping patterns that emerge under constraint. Yet many NCD strategies still under‑address the cognitive and structural pressures of urban life, leaving a critical gap in how we understand rising NCD burdens in LMIC cities.
Urbanisation is tightly linked to the NCD surge across African and Asian cities. When stressors are constant, the brain shifts into a state of hyper‑vigilance, a neurological adaptation with metabolic consequences. This is not simply a mental health issue; it is a biological pathway that connects the pressures of urban living to the rise in chronic disease.
Urban Stress as a Structural Exposure
For millions in LMICs, the city is a magnet for employment opportunities, yet these chronic stressors stem persistent, low-level anxiety of navigating unsafe informal settlements. Across LMICs, urban residents experience multiple overlapping stressors that influence their daily decisions and long‑term health.
Examples of this are seen in South Asia, where residents of Dhaka and Mumbai face chronic stress linked to overcrowding, heat, and insecure housing. In Southeast Asia, Jakarta’s extreme traffic congestion and long commuting times significantly increase stress and reduce the time available for food preparation. In Latin America, households in Mexico City and São Paulo experience high levels of food insecurity driven by income volatility and urban inequality. Similar patterns are seen in Cairo’s informal settlements, where housing precarity and environmental stressors shape diet quality and health. African cities such as Cape Town, Nairobi, and Accra show how transport systems, spatial inequality, and food access interact to influence diet‑related NCDs.
Figure 1: Chronic exposure to dense, high‑stimulation urban environments builds allostatic load, priming the body for metabolic and cardiovascular disease.
Cognitive Load: The Missing Mechanism
Chronic exposure to urban stressors reshapes the brain’s executive functions such as planning, impulse control, working memory, and decision‑making. Scarcity further reduces cognitive bandwidth, making it harder to plan ahead or prioritise long‑term health. At the same time, chronic stress disrupts cortisol rhythms, increasing cravings for high‑energy foods and elevating metabolic risk.
Neurologically, the amygdala becomes sensitised by repeated exposure to unpredictable, high‑pressure urban environment. This hyper‑arousal drives persistently high cortisol and inflammation, direct precursors to metabolic and cardiovascular disease.
These mechanisms are visible across LMIC cities. In India, irregular income and food insecurity push households toward cheap, filling foods. In Indonesia, long commutes and time poverty make convenience eating unavoidable. In Brazil and South Africa, stress and insecurity shape coping behaviours and ‘full stomach’ strategies. Across contexts, the pattern is consistent: urban stress alters neural function, constrains cognitive bandwidth, and shapes food choices, driving NCD risk long before clinical symptoms appear.
Food Choices Under Stress
Food choices in LMIC cities are deeply shaped by the interaction between stress, constrained cognitive bandwidth, and rapidly changing food environments. Ultra‑processed foods are expanding fastest in Latin America and Southeast Asia, driven by globalisation, supermarket growth, and aggressive marketing. UPFs are increasingly dominant in urban India, Indonesia, and the Philippines, where they are affordable, convenient, and heavily promoted. Across LMICs, time poverty, long commutes, and limited cooking fuel push households toward ready‑to‑eat foods. Skipping meals is common in food‑insecure households in South Asia, Africa, and Latin America, while limited refrigeration and high food prices reduce fruit and vegetable intake. These patterns are not simply preferences; they are structural responses to the pressures of urban living.
The Pathway From Stress to NCD Risk
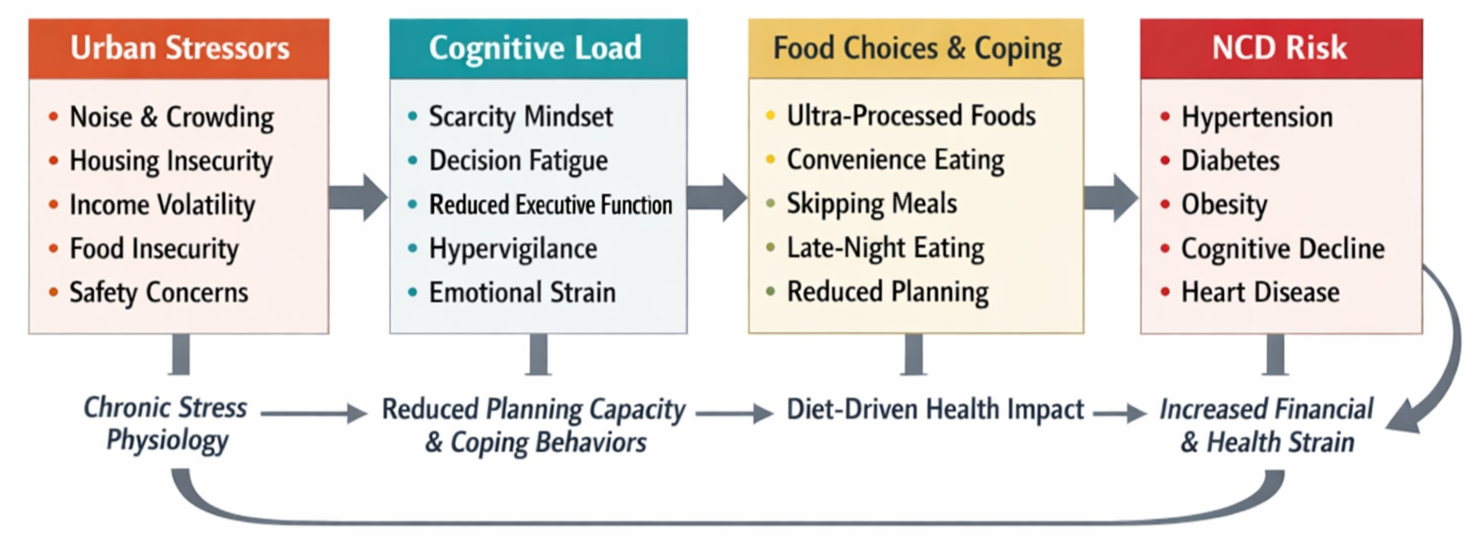
Evidence supports a clear, multi‑step pathway linking urban stress to NCD risk in LMIC cities. Structural stressors including housing insecurity, food insecurity, transport burdens, income volatility, violence, heat, and noise create chronic cognitive load. This reduces planning capacity, increases decision fatigue, and heightens emotional strain. Under these conditions, people rely on coping behaviours such as consuming ultra‑processed foods, skipping meals, or eating late at night. Over time, these patterns contribute to rising rates of hypertension, diabetes, obesity, and cardiovascular disease. This pathway aligns with global evidence that urbanisation and food system transitions are major drivers of NCDs in LMICs.
Why Current NCD Strategies Fall Short
Most NCD strategies still centre on downstream risk factors such as diet and physical activity, but they often under‑address the structural pressures that shape exposure and vulnerability. Evidence from LMIC contexts shows that food patterns are driven less by preference and more by constraints: transport, housing, income volatility, and the wider urban environment all shape stress and the conditions under which decisions are made.
Global policy analyses highlight that current NCD frameworks under‑address food environments and structural determinants, limiting their effectiveness in LMIC contexts. This creates a fundamental mismatch between policy assumptions and lived reality. As urban stress is environmental, it rarely appears on a blood panel or a glucose monitor. Consequently, interventions remain focused on the "end-stage" of the disease rather than the environmental causes. And as the vast majority of our data on urban stress comes from high-income settings. We lack a granular understanding of how these stressors manifest in the unique, resource-constrained, and high-density contexts of LMICs.
What this means for NCD policy in LMIC cities
These patterns point to several areas where policy needs to engage more directly with the systems shaping stress and exposure:
Urban planning must be integrated into NCD prevention, recognising that transport systems, housing conditions, and neighbourhood infrastructure, as well as the sensory environment of noise, heat, and crowding, shape food access and stress exposure.
Food system governance must address the rapid penetration of ultra‑processed foods in LMIC markets, alongside policies that reduce stress‑driven consumption patterns and stabilise access to affordable, nutritious foods.
NCD strategies must incorporate cognitive load, acknowledging that behaviour‑change models fail when people lack the bandwidth to plan or prioritise health. This includes health communication that recognises cognitive fatigue and social protection measures that stabilise income and food access.
Evidence from Africa, Asia, and Latin America shows that city‑level, intersectoral interventions such as those piloted in the Nourishing Spaces project can address the structural drivers of diet‑related NCDs.
To be effective, global NCD strategies must integrate urban systems, food environments, and the cognitive realities of daily life. This is the missing link in global NCD prevention.
We cannot solve the LMIC NCD crisis by only looking at what people put into their bodies i.e. food or smoking. We must also analyse what the environment puts into their brains. Ignoring the neural architecture of urban stress guarantees that NCD strategies will fall short.
A man with his bicycle stacked with fruit and vegetables in Kathmandu, Nepal from unsplash


A man sitting next to rumble, waiting to sell at his food stand as people walk by in Bangladesh from unsplash